Pneumonia

A child dies of pneumonia every 43 seconds
Pneumonia kills more children than any other infectious disease, claiming the lives of over 700,000 children under 5 every year, or around 2,000 every day. This includes around 190,000 newborns. Almost all of these deaths are preventable. Globally, there are over 1,400 cases of pneumonia per 100,000 children, or 1 case per 71 children every year, with the greatest incidence occurring in South Asia (2,500 cases per 100,000 children) and West and Central Africa (1,620 cases per 100,000 children).
Progress in reducing deaths due to pneumonia in children under 5 has been significantly slower than for other infectious diseases. Since 2000, under-five deaths due to pneumonia have declined by 54 per cent, while deaths due to diarrhoea have decreased by 63 per cent and are now almost half of pneumonia deaths.
Mortality due to childhood pneumonia is strongly linked to poverty-related factors such as undernutrition, lack of safe drinking water and sanitation, indoor and outdoor air pollution as well as inadequate access to health care. An estimated 18 million more health workers are needed by 2030 to prevent, diagnose and treat pneumonia to reach the Sustainable Development Goal targets on universal health coverage.
Around half of childhood pneumonia deaths are associated with air pollution. The effects of indoor air pollution kill more children globally than outdoor air pollution. At the same time, around 2 billion children 0–17 years of age live in areas where outdoor air pollution exceeds international guideline limits.
Early care-seeking for children with acute respiratory infection (ARI) symptoms from a health care provider is known to reduce mortality, yet population-based survey data indicate that there has been slow progress in care-seeking behaviour for children with ARI. In the last decade, seeking care for children with ARI symptoms from a healthcare provider has stagnated in many regions and declined in South Asia and the Middle East and North Africa. Pneumonia is an ARI of the lungs. Globally, less than two thirds (60 per cent) of children with symptoms of ARI were taken to a health care provider in 2024. Although it cannot be assumed that all children with symptoms have bacterial ARI and should receive antibiotics, the data indicate a gap in the likelihood of treatment between the richest and the poorest (68 per cent and 50 per cent, respectively). Furthermore, in sub-Saharan Africa, where the most pneumonia deaths occur, only around 50 per cent of children with ARI symptoms are taken for care.
Simple solutions can save children’s lives
The Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea (GAPPD) sets forth an integrated framework of key interventions proven to effectively protect children’s health, prevent disease and appropriately treat children who fall ill with diarrhoea and symptoms of pneumonia.
Protect, prevent and treat framework on diarrhoea and acute respiratory infection
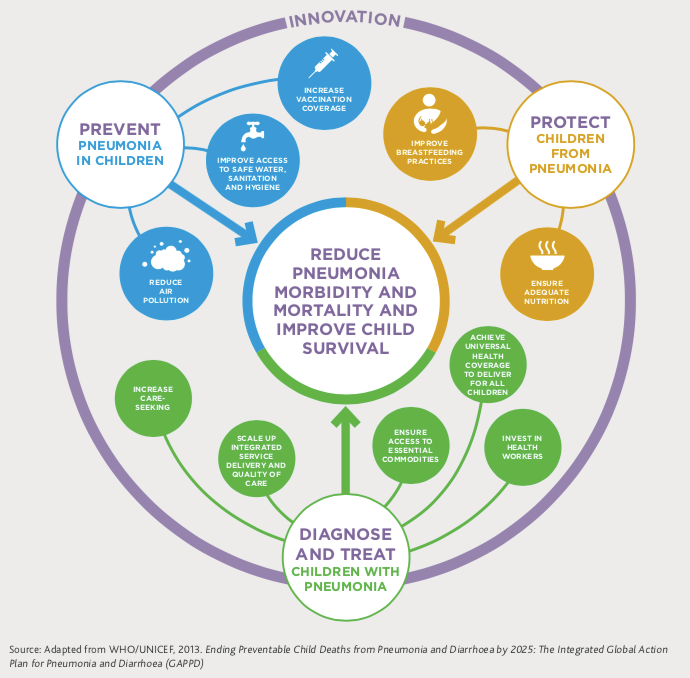
Protect: Protective interventions provide the foundations for keeping children healthy and free of disease
- Exclusive breastfeeding for the first 6 months of life (without additional foods or liquids, including water) protects infants from disease and guarantees them a food source that is safe, clean, accessible and perfectly tailored to their needs. Nearly half of all diarrhoea episodes and one-third of all respiratory infections could be prevented with increased breastfeeding in low- and middle-income countries.
- Adequate complementary feeding and continued breastfeeding provides good nutrition, supports strong immune systems and provides protection from disease. From 6 months to 2 years of age, adequate complementary feeding —providing children with adequate quantities of safe, nutritious and age-appropriate foods alongside continued breastfeeding — can reduce child deaths, including those due to pneumonia and diarrhoea.
Prevent: Preventative interventions help stop disease transmission and prevent children from becoming ill
- Immunization: The Haemophilus influenzae type b (Hib) and pneumococcal conjugate vaccines (PCV) are effective in preventing the two most common bacterial causes of childhood ARI, including pneumonia. In addition, the use of vaccines against measles and pertussis in national immunization programmes substantially reduces ARI and death in children. In 2024, 42 million infants did not receive the recommended three doses of PCV, putting them at higher risk of ARI.
- Reduced household air pollution: Around a third of the world’s population rely on solid fuels (wood, coal, animal dung and crop waste) to cook and heat their homes, exposing children to household air pollution and almost doubling their risk of developing an ARI. Improved household air quality can reduce cases of severe ARI while also preventing burns, saving time and reducing fuel costs. The use of chimney stoves can cut household air pollution by half, reducing the risk of developing severe ARI by almost 30 per cent.
- HIV prevention: Preventing HIV and treating HIV infections with antiretroviral drugs helps maintain the immune system and reduce the risk of contracting ARI. Co-trimoxazole prophylaxis provides further ARI-related protection for HIV-infected and exposed children and can reduce AIDS deaths by 33 per cent.
Diagnose and Treat: Treatment interventions – when timely and appropriate – can cure children from pneumonia and ensure survival
Saving children from ARI requires urgent action; the first step is recognizing danger signs (including fast and difficult breathing and a cough). The treatment for most types of serious ARI is often antibiotics, which typically cost less than 50 cents for a full treatment. However, not all children with ARI symptoms should receive antibiotics. According to the WHO and UNICEF Integrated Management of Childhood Illness guidelines, only those cases classified by a health worker as pneumonia or severe ARI should be treated with antibiotics. Moreover, not all children classified as such have true ARI. That said, in settings without adequate diagnostic tools, the WHO/UNICEF guidelines provide a common standard by which health workers can assess and classify bacterial ARIs requiring antibiotic treatment.
References
IEA, IRENA, UNSD, World Bank, WHO, Tracking SDG 7: The Energy Progress Report, World Bank, Washington, DC, 2022.
UNICEF, One is too many: Ending child deaths from pneumonia and diarrhea, UNICEF, New York, 2016.
UNICEF, Clean the air for children, UNICEF, New York, 2016.
UNICEF, Committing to Child Survival: A promise renewed – Progress report 2015, UNICEF, New York, 2015.
United Nations Inter-agency Group for Child Mortality Estimation (IGME), Child mortality, stillbirth, and causes of death estimates, WHO and UNICEF, New York, 2024.
Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025: The integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD), WHO, Geneva, 2013.
UNICEF, Pneumonia and Diarrhoea: Tackling the deadliest diseases for the world’s poorest children, UNICEF, New York, 2012.
WHO and UNICEF, Global Action Plan for the Prevention and Control of Pneumonia (GAPP): Report of an informal consultation, WHO, Geneva, 2008.
WHO and UNICEF, Integrated Management of Childhood Illness, WHO, Geneva, 2008.
UNICEF and WHO, Pneumonia: The forgotten killer of children, UNICEF, New York, 2006.
Peer-reviewed Publications
Villavicencio, Francisco et al. (2024), ‘Global, regional, and national causes of death in children and adolescents younger than 20 years: an open data portal with estimates for 2000-21’, The Lancet Global Health, Volume 12, Issue 1, e16-e17.
Campbell, H., et al., ‘Measuring Coverage in MNCH: Challenges in monitoring the proportion of young children with pneumonia who receive antibiotic treatment’, in PLOS Medicine: published 7 May 2013, info:doi/10.1371/journal.pmed.1001421 (see: PLOS Collection: Measuring Coverage in Maternal, Newborn, and Child Health).
Child Health
Resources






Notes on the Data
KEY TERMS
Acute respiratory infection (ARI): This includes any infection of the upper or lower respiratory system, as defined by the International Classification of Diseases. Acute lower respiratory infections (ALRI) affect the airways below the epiglottis and include severe infections, such as pneumonia.
Pneumonia: Pneumonia is a severe form of acute lower respiratory infection that specifically affects the lungs and accounts for a significant proportion of the ALRI disease burden. The lungs are composed of thousands of tubes (bronchi) that subdivide into smaller airways (bronchioles), which end in small sacs (alveoli). The alveoli contain capillaries where oxygen is added to the blood and carbon dioxide is removed. With pneumonia, pus and fluid fill the alveoli in one or both lungs, and this interferes with oxygen absorption, making breathing difficult.
Symptoms of pneumonia: Signs of pneumonia are a combination of respiratory symptoms, including ‘cough and fast or difficult breathing due to a chest-related problem’. Children exhibiting such symptoms should be taken to a health provider for a clinical assessment for pneumonia. Not all children with symptoms of pneumonia should receive antibiotic treatment; only children with a confirmed case of pneumonia (classified as such by the Integrated Management of Child Illness guidelines and based on a rapid respiratory rate counted by a health worker) should receive them. Current pneumonia-related interventions at the population level are measured through household surveys. However, evidence indicates that it is not possible to measure pneumonia prevalence among children under age 5 during a household survey interview or to ascertain underlying pneumonia for children with these respiratory symptoms.
Measurement limitations: Data collected through national household surveys, such as Multiple Indicator Cluster Surveys (MICS) and Demographic and Health Surveys (DHS), report on the prevalence of symptoms of pneumonia, based on information about whether children have experienced coughing and fast or difficult breathing (due to a problem in the chest) in the two weeks prior to the survey. These children have not necessarily been medically diagnosed, and thus these data should be interpreted with caution. This limitation affects the accurate measurement of the coverage indicator on treatment of symptoms of pneumonia with antibiotics. The indicator becomes underestimated due to inflation of the denominators with children with apparent symptoms of pneumonia, but who did not actually have pneumonia, and therefore were not treated with antibiotics.